Inclusivity is a vital aspect of clinical trials and data collection, necessitating the active involvement of patients and healthcare professionals in their design. A study comparing the trialists’ choice of primary outcome with what patients and health professionals want found that the primary outcome in a trial was only ranked as the most important outcome by patients and health professionals 28% of the time out of the 44 trials sampled. Considering that the primary outcome in a trial is the most important piece of data collected, it becomes imperative to seek input from patients and healthcare professionals to ensure the relevance and utility of the measured outcome.
An additional study re-examined the same sample of trials to check if any of them had Patient and Public Involvement (PPI) in the selection of collected outcomes, finding that none did. Emphasising PPI in this context can be an effective means of ensuring that clinical trials address the needs of patients effectively.
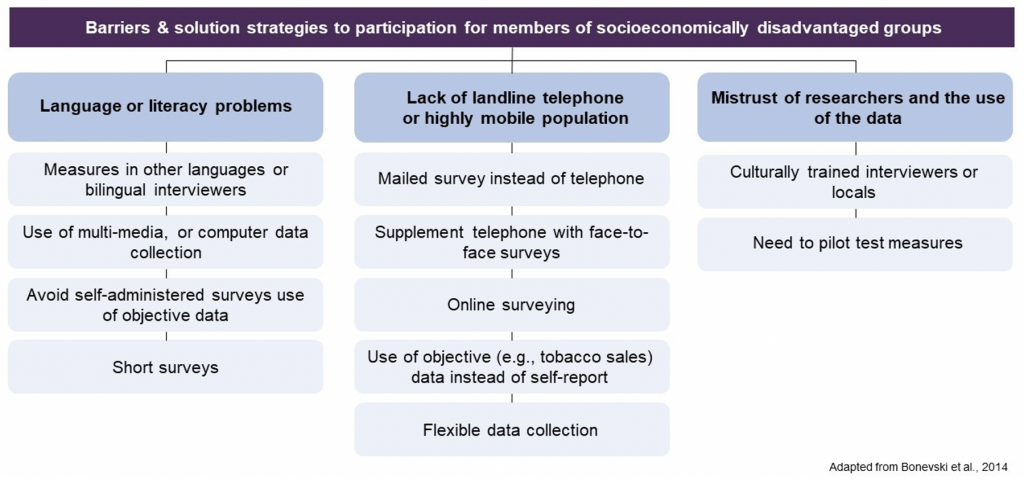
Furthermore, it is important to consider how data collection and measurement methods might inadvertently create barriers for individuals from socioeconomically disadvantaged groups. A literature review on this subject yielded a list of data collection improvements (see image below). In summary, the review underscored the significance of acknowledging extended timeframes, allocating higher resourcing costs, and fostering community partnerships to enhance the representation of socially disadvantaged groups in clinical trials.
To promote inclusivity, there are also valuable guidelines available for posing questions on sensitive topics:
- Ethnicity harmonised standard – UK government standards for collecting ethnicity data.
- Equality, Diversity and Inclusion in Science and Health survey question guidance